Introduction:
Myopia is the most widespread refractive condition and one of the primary causes of vision impairment globally. Geographically, the prevalence of myopia varies. High myopia being strongly connected to increased risk of ocular comorbidities. As a result, preventing myopia progression is an important public health concern. Pharmaceutical medications, bifocal lenses, multifocal lenses, aberration control spectacle lenses, and soft and gas-permeable contact lenses have all been introduced to reduce the progression of myopia.
Orthokeratology (ortho-k) is the practise of purposely restructuring the anterior cornea with customised contact lenses to minimise refractive error temporarily and reversibly following lens removal. These are gas permeable contact lenses used to correct refractive errors such as myopia, hyperopia, and astigmatism. Modern ortho-k incorporates reverse geometry lens designs comprised of high oxygen permeable rigid materials that are worn overnight to reshape the anterior cornea and deliver temporary refractive correction. Ortho-k has lately been widely utilised to reduce the incidence of myopia in youngsters. Since they rectify the refractive defect momentarily, these lenses eliminate the need for glasses or contact lenses during the day. The effect usually lasts 10-12hours after waking until the cornea returns to its natural form. Modern ortho-k lenses can temporarily correct up to -6D of myopia, up to -1.50 D of astigmatism.
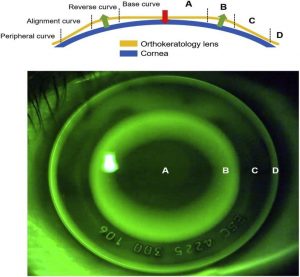
Fig 1: Spherical Ortho-k lens design in-situ [Source: Vincent, S. J., Cho, P., Chan, K. Y., Fadel, D., Ghorbani-Mojarrad, N., González-Méijome, J. M., … & Jones, L. (2021). BCLA CLEAR-Orthokeratology. Contact Lens and Anterior Eye, 44(2), 240-269.]
Effect of ortho-k lenses on refractive errors:
The ortho-k lens’s reverse geometry design moulds the cornea of a myopic eye into a plateau form. These orthokeratology lenses have a much flatter central base curve, resulting in positive pushing pressure against the central cornea and negative pulling pressure against the mid-periphery, redistributing epithelial cells to the mid-periphery while flattening the central cornea via epithelial layer thinning. Light would be refracted simultaneously into the mid-peripheral retina and macula through a plateau-shaped cornea, leaving the peripheral retina with relative myopic defocus. On the other hand, hyperopic peripheral defocus, which is common in myopic children, is thought to promote eye development. It is predicted that manipulating peripheral defocus toward myopia will stabilise eye development and slow the evolution of myopia.
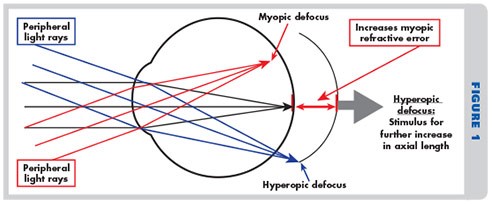
Fig 2: Peripheral defocus and myopia progression [Source: Eyedolatry: What’s Happening to Our Vision? Peripheral Defocus and Myopia Progression [Internet]. Eyedolatry. 2022 [cited 13 March 2022]. Available from: https://www.eyedolatryblog.com/2015/06/whats-happening-to-our-vision.html]
Several studies have suggested that ortho-k lenses can slow the progression of myopia by 85-93.5 percent. In 2007, a two-year study (CRAYON) was conducted in the United States with 28 children aged 7 to 11 years old, some of whom wore soft lenses and others ortho-k lenses. The results showed that children wearing ortho-k lenses had their axial length elongation reduced by 0.16mm and their vitreous chamber depth reduced by 0.10mm within a year. Another study conducted in Australia (CRIMP) compared 32 children wearing ortho-k lenses to 32 children wearing spectacles over 10 years and discovered that 70% of the children wearing ortho-k lenses did not experience progression of myopia.
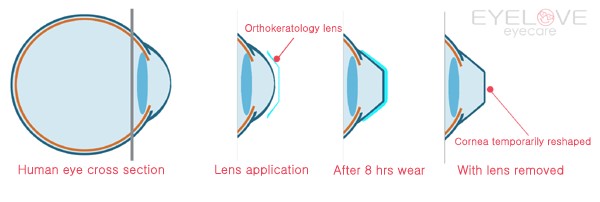
Fig 3: Effect of ortho-k lenses on cornea [Source: Ortho-k lens Orthokeratology [Internet]. Iloveicare.co.nz. 2022 [cited 13 March 2022]. Available from: http://www.iloveicare.co.nz/services/Orthokeratology.html]
In hyperopia, however, the ortho-k lens is not as effective as it is in myopia. Ortho-k for hyperopia relies on paracentral corneal thinning rather than a combination of paracentral and central corneal thinning. The majority of ortho-k lenses for astigmatism correction for with the rule astigmatism are available up to 1.75D. A study for toric ortho-k included children with the myopia of up to 5D and with the rule astigmatism of 1.25to 3.50D after wearing these lenses for 1-month astigmatism was reduced by 79% and myopia was reduced by 81%. The usage of ortho-k lenses helps correct mild to moderate myopia, but not for hyperopia or presbyopia.
Conclusion:
Orthokeratology is a safe treatment that can help achieve good vision and slow the progression of myopia. It is gaining popularity, particularly among youngsters who have witnessed the benefits of myopia management. It is well-liked by both practitioners and patients. Specialized training, equipment, and skills are required. Over the previous 30 years, ortho-k lenses have improved in terms of lens structure and design, as well as lens materials. To correct the excessive quantity of myopia and astigmatism, further clinical research and development in the design of these lenses is required.
Shivani Mishra; RoshniSengupta